

Abstract
Introduction: Chimeric antigen receptor (CAR) T-cell therapy has displayed potent anti-leukemia activity in refractory/relapsed acute lymphocytic leukemia (ALL). However, the influence of CAR-T therapy on host systemic and local immunity has not been well examined. We therefore applied high-throughput T cell receptor β chain sequencing to track dynamic change of T-cell repertoire in vivo induced by CAR-T therapy in B-cell acute lymphocytic leukemia patients.
Patients and Methods: Six patients with 45 samples were under observation. The samples obtained to be tested were the peripheral blood mononuclear cell (PBMC) samples and bone marrow mononuclear cell (BMMC) samples before and after CAR-T administration, as well as the CAR-transduced autologous T cell samples on the day when they were to be infused to patients. The information of samples and patients was summarized in Table 1. The TCR full length mRNAs of these samples were deeply sequenced using the ImmunHubTM TCR profiling system (ImmunQuad Biotech). Briefly, a 5'RACE unbiased amplification protocol was used. An algorithm was applied to raw sequencing data for PCR and sequencing errors correction and V, D, J, C gene segments mapping with IMGT®. The inverse Simpson index and the clonality index was calculated to estimate TCRβ clonotype diversity and the state of clonal proliferation of T cells. The donut chart and clone tracking heat map were generated by R.
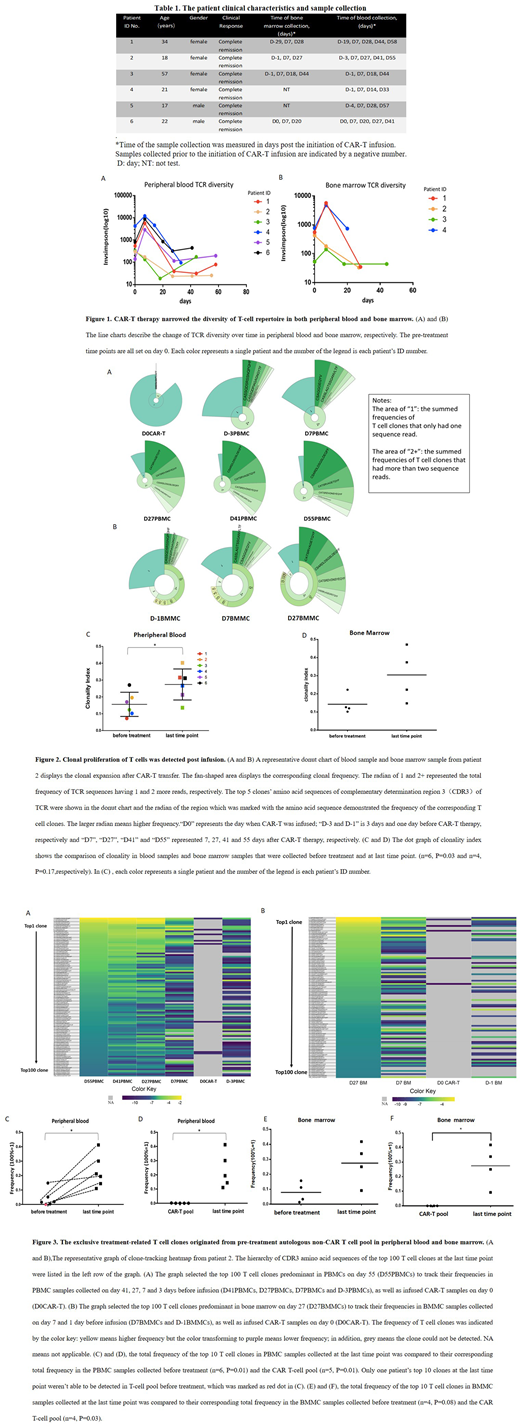
Result: Compared to preinfusion TCR diversity, we observed inverse Simpson's index of 4 of 6 patients' PBMC samples (Fig. 1A) and of 3 of 4 patients' BMMC samples (Fig. 1B) had been increasing to day 7 after CAR-T treatment. As time went by, a decline of TCR diversity from day 7 to day 28 was detected in both PBMC and BMMC samples (Fig. 1). Of note, a relative rising tide of TCR diversity was observed after the decline in PBMC samples (Fig. 1A). The decreased TCR diversity leaded us to test the change of TCR clonality. As shown by Fig. 2A and 2B, in comparison with the pre-treatment and the CAR-T samples, we detected highly clonal proliferation of T cells in both blood and bone marrow. Next, we applied the clonality index to quantitatively define T cell clonal expansion (Fig. 2C and 2D). The clonality index was raised from 0.16±0.07 and 0.14±0.05 before treatment to 0.27±0.09 and 0.3±0.15 at last time point post infusion in PBMCs and BMMCs, respectively (mean ± SD, student's t test, P=0.03 and P=0.17, respectively).CAR-T-induced T-cell clonal expansion triggered us to trace back the original clonal source. For tracking clonal evolution, we selected the 100 most prevalent T cell clonotypes found at the last time point in both PBMCs and BMMCs and tracked their frequencies at earlier time points. As was displayed by the heat map, the top 100 T cell clones dominating in PBMCs and BMMCs at the last time point were barely found in CAR-T cell pool and were the low-frequency clonotypes in preinfusion samples (Fig. 3A and 3B). In order to quantitatively describe this phenomenon, we compared the total frequency of top 10 T cell clones in PBMC and BMMC samples at the last time point to their corresponding total frequency in preinfusion samples and the infused CAR-T pool (Fig. 3C, 3D, 3E and 3F). The total frequency of the top 10 T cell clones was 23%±11% and 27%±14% at last time point, 4%±6% and 8%±7% before treatment and 0.05%±0.09% and 0.01%±0.01% in the infused CAR-T samples in PBMCs and BMMCs, respectively (mean ± SD, Fig. 3C, 3D, 3E and 3F; student's t test, P=0.01, P=0.01, P=0.08 and P=0.03, respectively). Only one patient's (patient 6's) top 10 T cell clones in PBMCs at last time point were not found in both CAR-T pool and preinfusion sample, which may be caused by the limitation of sequencing detection (Fig. 3C).
Conclusion: For the first time, we demonstrated CAR-T therapy could stimulate the clonal proliferation of endogenous non-CAR T cells in patients. Along with other groups' animal results (Barber A et al. J Immunol. 2009) indicating that CAR-T therapy could facilitate the infiltrating of tumor antigen-specific T cells, these expanded T cell clones of patients in our trial are most likely tumor antigen specific, which could provide synergistic anti-tumor effect following CAR-T adoptive transfer. The trial was registered in Chinese Clinical Trial Registry and the registration number is ChiCTR-OCC-15007008.
No relevant conflicts of interest to declare.

